Re-entry of the impulse (re-entry mechanism). Re-entry in poker - what is it? Arrhythmias by type re entry
Includes two main mechanisms - re-entry and violation of intracardiac hemodynamics.
Re-entry mechanism in arrhythmia
One of the main mechanisms of the pathophysiology of arrhythmias, the ways of developing tachyarrhythmias, extrasystole is considered the mechanism of the formation of re-entry of excitation - the re-entry mechanism. The re-entry is based on the circulation of the excitation wave along repeating trajectories in the myocardium. It is generally accepted that the form of such movement is a ring, however, studies show that this form has a more complex spatial orientation.
In accordance with the theory of re-entry, it is assumed that there are shunts (shunt bridges) between the branches of the Purkinje fibers. The re-entry mechanism is explained as follows. Imagine that in one of the branches of the Purkinje fibers, the movement of the impulse in the distal direction is disturbed, but the retrograde conduction of the impulse is preserved. In this situation, the impulse in the distal direction will only travel along a normally functioning fiber. The presence of shunt bridges allows the impulse to enter the branch with impaired impulse conduction in the distal direction just in its distal section (end). The pulse entry time is characterized by a certain delay (the delay time is equivalent to the time required for this section to exit the refractory state). The retrograde movement of the impulse and the subsequent repetition along the shortened path will lead to premature contraction of the myocardium.
Thus, for the circulation of excitation, a unidirectional blockade of impulse conduction is necessary. This theory, first formulated by Th. Lewis in 1925, was significantly supplemented in subsequent years, in particular, the concept of the necessary mass of the myocardium sufficient for the re-entry wave, ways to stop this mechanism (prolongation of refractoriness), local changes in unidirectional blockade of conduction to bidirectional. Clinical arguments in favor of the re-entry mechanism can be considered the constancy of the clutch interval in cases of the same ectopic focus and a clear relationship between the appearance of extrasystoles and the heart rate (HR), which determines a strictly defined duration of the refractory period.
Understanding the mechanisms of the pathophysiology of arrhythmia and the circulation of excitation waves led to the creation of a new direction in interventional cardiology - interventional arrhythmology. Thus, interruption of multiple paths of circulation of excitation in the left and right atria (LA and RA) by dissecting them into several separate fragments (“labyrinth”) leads in some cases to the cessation of MA.
Violation of intracardiac hemodynamics in arrhythmias
The mechanism of the pathophysiology of re-entry arrhythmias described above suggests that if an ectopic focus is located in one of the ventricles, the excitation caused by it can spread retrogradely through the conduction system of the heart and reach the AV connection earlier than the wave of normal excitation from the sinus node. This will cause the AV junction to be in the refractory phase when it is reached by normal excitation from the sinus node. Thus, the conduction of the impulse into the ventricles will become impossible, which will lead to the loss of the next contraction of the ventricles. In such a situation, an extended diastolic pause (compensatory pause) will occur. With PVC, the sum of the intervals during extrasystole and after extrasystole shows that the value obtained is equal to the sum of two normal cardiac cycles. Such a compensatory pause is called complete. It is important to note that the contraction following the extrasystole is always stronger than the previous one (the effect of post-extrasystolic potency).
Extrasystoles, even frequent (>6 per 1 min), do not lead to a change in intracardiac hemodynamics if the myocardium is preserved, i.e. there are no focal or diffuse changes in it. In the presence of myocardial damage, compensatory mechanisms (compensatory pause and the effect of post-extrasystolic potency) cannot prevent a decrease in cardiac output. It is important to note that with extrasystoles, tachycardias, the duration of diastole changes first of all, which leads not only to uneven force of contraction of the ventricles, but also to filling the ventricles with different volumes. At the same time, the “stiffness” of the myocardium increases, which makes it difficult to fill the ventricular cavities in the next cycle. Changing the duration of diastole also leads to an inadequate decrease in myocardial blood flow.
The result of such changes is a violation of the transmitral and transtricuspid blood flow, an increase in atrial pressure, “stagnation” in the pulmonary circulation, and a decrease in stroke volume (SV). Thus, any rhythm disturbances that occur against the background of existing morphological changes in the myocardium lead to the development of increased myocardial stiffness, which contributes to stagnation in the pulmonary circulation and exacerbates the course of circulatory failure.
Such changes in intracardiac hemodynamics in the pathophysiology of arrhythmias lead to an increase in total peripheral vascular resistance (TPVR), which, in turn, reduces the ejection fraction (EF). The described hemodynamic changes very quickly lead to systemic changes, as they include neurohormonal changes in the pathological process: an increase in the activity of norepinephrine, angiotensin II (ATP) and plasma renin.
The article was prepared and edited by: surgeonArrhythmias are initiated and maintained by a combination of the occurrence of an abnormal impulse (action potential) and the conduction of an abnormal impulse. The generation of normal and abnormal impulses is known as automatism. Conduction of an impulse is called normal or abnormal, depending on the way it is transmitted: orthograde path - normal conduction; according to the reentry mechanism - abnormal, or blocked, conduction. Automatism can initiate an arrhythmia if it occurs ectopically (outside the place of usual localization, i.e. not in the SA node).
Examples of arrhythmias, apparently caused by automatism, can serve as:
nodal tachycardia.
PVCs associated with developing myocardial infarction.
There are three types of automation which can lead to:
increased normal automatism occurs in tissues (AV node and bundle of His) capable of slow automatic generation of impulses, which under normal conditions is overridden by more frequent impulses from the SA node. Normal automatism can be enhanced under the influence of drugs and diseases;
abnormal automatism occurs in tissues that are incapable of automatic generation of impulses under normal conditions (ie, atrial or ventricular). During pathological processes (for example, in myocardial infarction), abnormal automatism often occurs in Purkinje fibers. Catecholamines may enhance this type of automatism;
trigger automatism (known as trigger activity) is similar to abnormal automatism, but here the aberrant impulses are generated prior to the normal impulse. There are two types of trigger activity. Early post-depolarization (EPD) occurs during the repolarization phase of the action potential (i.e., during phase 2 or 3). RPD is increased under the influence of bradycardia and drugs that increase the duration of the action potential (for example, class III antiarrhythmic drugs). The mechanism underlying RPD is unknown.
Excitation spreads from "a" towards "b" and "d". Due to the blockade of conduction and the refractory period in the "d" fiber, the excitation spreads along the "" fiber and causes systole.
If there is a unidirectional blockade, ie. If the propagation of excitation in one direction is blocked, for example, in the antegrade direction, then the excitation after the end of the refractory period in the opposite direction reaches the “d” fiber.
Systole sets in, more precisely, ventricular extrasystole, but if a circular motion of the excitation wave occurs, then an attack of ventricular tachycardia appears.
Delayed post-depolarization(APD) occurs after the end of the action potential (i.e. during phase 4). In typical cases, PPD appears as a result of intracellular Ca2+ ion overload, which can occur during AMI, reperfusion, or digitalis intoxication. Ca2+ overload leads to a pulsatile release of Ca2+ from the sarcoplasmic reticulum and the generation of an inward current (which leads to RPD) carried by the Ca+/Ca2+ exchanger.
Re-entry mechanism and blockade of conduction - conditions for the occurrence of arrhythmias. The most common site of heart block is the AV node:
with AV blockade of the 1st degree, conduction through the AV node is slowed down, which manifests itself on the ECG as a prolongation of the PR interval;
AV blockade of the II degree is characterized by the absence of some impulses in the ventricles (i.e., their contraction does not occur). On the ECG, the QRS complex does not always follow the P wave;
AV block III degree (complete) is clinically the most severe. Completely stops conducting impulses at the level of the AV node. This leads to a slowing down (delay) of the ventricular contraction rate, which does not provide adequate cardiac output. Aberrant conduction of this type can unmask zhes.
Re-entry mechanism supports (and can initiate) ventricular tachycardia and ventricular fibrillation. The re-entry mechanism is conduction circulation with repeated tissue re-excitation in the absence of a diastolic interval. In 1914, Meine identified the conditions for the occurrence of re-entry: the presence of a site of unidirectional blockade of the impulse, which makes it possible to reverse (retrograde) conduction with re-excitation of the tissue bypassing the block. The following criteria indicate the existence of a reentry mechanism:
the length of the conduction path is greater than the wavelength (co) determined by the effective refractory period (ERP) and conduction velocity (CV), i.e. to = ERP x CV;
the presence of a unidirectional blockade of conduction.
Unidirectional blockade conduction may be anatomic (as in Wolff-Parkinson-White syndrome) or functional (eg, prolonged refractoriness resulting from ischemia); both factors can be present at the same time. Re-entry can be interrupted by premature activation, artificial acceleration of the heart rate and the introduction of drugs. The re-entry mechanism plays a role in maintaining and possibly initiating atrial tachycardia, atrial fibrillation, AV nodal tachycardia, Wolff-Parkinson-White syndrome, ventricular tachycardia, and ventricular fibrillation.
Classification of arrhythmias
ASSOCIATED WITH AUTOMATIC DISTURBANCES
A. Violations of the automatism of the sinus node
Sinus tachycardia
Sinus bradycardia
sinus arrhythmia
Sick sinus syndrome
B. Ectopic rhythms (heterotopic arrhythmias)
atrial rhythm
Nodal (atrioventricular) rhythm
Idioventricular (ventricular) rhythm
Migration of the supraventricular pacemaker
Atrioventricular dissociation
RELATED TO EXCITABILITY DISTURBANCES
Extrasystole
Paroxysmal tachycardia
ASSOCIATED WITH IMPAIRMENT OF EXCITABILITY AND CONDUCTIVITY
Atrial fibrillation (fibrillation) (atrial fibrillation)
atrial flutter
Flutter and fibrillation (flicker) of the ventricles
CONDUCTIVITY RELATED
Sinoatrial blockade
Intra-atrial block
Atrioventricular block
Intraventricular blockade (blockade of the branches of the bundle of His).
Syndromes of premature excitation of the ventricles
a) Wolf-Parkinson-White syndrome (WPW).
b) Syndrome of the shortened PQ interval (CLC).
the occurrence of arrhythmia according to the mechanism: early and late postdepolarization, macro- and micro-re-entry.
1) EARLY POST-DEPOLARIZATION- this is a premature depolarization of myocardial cells and the conduction system, which appears when the repolarization phase of the action potential has not yet been completed, the membrane potential has not yet reached the resting potential. This premature AP is considered to be triggered (induced) because it owes its onset to early post-depolarization emanating from the main AP. In turn, the second (induced) AP, due to its early post-depolarization, can cause a third, also trigger AP, and the third AP - the fourth trigger AP, etc. If the source of trigger activity is in the ventricles, then on the ECG a similar type of disturbance in the formation of impulses manifests itself as ventricular extrasystole or polymorphic ventricular tachycardia.
You can specify two of the most important conditions for the occurrence of early post-depolarizations, such as: prolongation of the repolarization phase of the action potential and bradycardia. With a slowdown in repolarization and, accordingly, an increase in the total duration of AP, premature spontaneous depolarization may occur at a time when the repolarization process has not yet been completed. With a decrease in the frequency of the main heart rhythm (bradycardia), there is a gradual increase in the amplitude of early postdepolarizations. Having reached the threshold of excitation, one of them causes the formation of a new AP even before the completion of the original one.
Since early post-depolarizations are realized due to the activation of Na + - and Ca2 + channels, it is possible to suppress the associated cardiac arrhythmias with the help of blockers of these channels.
The occurrence of early post-depolarizations is facilitated by: hypercatecholaminemia, hypokalemia, acidosis, ischemia, long QT syndrome. Often, such automatism is the result of the use of antiarrhythmic drugs that block K + channels (sotalol, quinidine, etc.).
2) LATE (DELAYED) POST-DEPOLARIZATIONS- this is a premature depolarization of myocardial cells and conductive tissue, which appears immediately after the completion of the repolarization phase. Occur, as a rule, after partial hyperpolarization (trace potentials). If the post-depolarization amplitude reaches the AUD, AP occurs, etc. Subthreshold fluctuations in the membrane potential, which can normally be present, but never manifest themselves, under pathological conditions that cause Ca2+ overload of cardiomyocytes, can increase in amplitude, reaching the threshold of excitation.
An increase in the intracellular concentration of calcium ions causes the activation of non-selective ion channels, which provide an increased supply of cations from the extracellular environment to the cardiomyocyte. At the same time, mainly Na+ ions enter the cell, the concentration of which in the extracellular fluid is much higher than the level of K+ and Ca2+. As a result, the negative charge of the inner surface of the cell membrane decreases, reaching a threshold value, followed by a series of premature APs. Ultimately, a chain of trigger excitations is formed.
Trigger activity of heart cells associated with delayed post-depolarizations can occur under the action of cardiac glycosides or catecholamines. Very often it appears with myocardial infarction.
3)For the formation of MACRO RE-ENTRY with its characteristic properties, certain conditions are required:
The presence of a stable closed loop, its length depends on the anatomical perimeter of the non-excitable obstacle around which the impulse moves;
Unidirectional blockade of conduction in one of the segments of the re-entry loop;
The duration of the propagation of the excitation wave must be shorter than the time during which the impulse can travel the entire length of the re-entry loop. Due to this, in front of the front of the pulse propagating in a circle, there is a tissue section that has left the state of refractoriness and has managed to restore its excitability (“window of excitability”).
The mechanism of macro reentry is believed to underlie atrial flutter.
This circulation can be eliminated by lengthening the refractory period. In this case, the “window of excitability” may close, since the circulating wave encounters a region that is in a state of refractoriness. This can be achieved with the help of antiarrhythmic drugs that block K + channels, which leads to a slowdown in repolarization and an increase in the duration of the refractory period. In this case, the "window of excitability" closes, and the movement of the impulse stops.
4) With MICRO RE-ENTRY the movement of the impulse occurs along a small closed ring, not associated with any anatomical obstacle. The impulse makes not only circular, but also centripetal motion. Closer to the center, AP decreases, and excitation fades, cells in the center give only a local response, because are in a state of refractoriness and, as it were, replace an anatomical obstacle.
Apparently, many complex tachyarrhythmias, in particular fibrillations, are associated with the micro re-entry mechanism. Combinations of loops lying in different planes occur in patients with ventricular tachycardia in the acute period of myocardial infarction.
Very often, the morphological substrate for the occurrence of re-entry is the Purkinje fibers located in the ischemic zone. These cells are resistant to hypoxia and may not die in the focus of infarction. However, at the same time, they change their electrophysiological characteristics in such a way that fast Na+ channels turn into “slow” ones. In this case, the conduction of the impulse slows down and it leaves the ischemia zone at the moment when the rest of the myocardium is already in a state of relative refractoriness and is ready for re-excitation, but the impulse from the sinus node has not yet arrived. The phenomenon of re-entry occurs when the myocardium is stimulated twice by the same impulse: the first time when it enters from the sinus node, and the second time when it re-emerges from the ischemic zone. In this case, it is possible to break the re-entry loop with the help of drugs that block "slow" Na + channels in the ischemic zone (lidocaine, novocainamide).
The undoubted advantage of these antiarrhythmics is that they show a high affinity specifically for abnormal Na+ channels in the ischemic zone and practically do not inhibit fast Na+ channels in healthy myocardial cells, and therefore do not affect electrophysiological processes in intact cardiomyocytes.
The following factors lead to a violation of the conduction of an impulse in the heart:
1. Reducing the magnitude of action potentials.
2. Slowing down the propagation of the generated impulse to unexcited cells (for example, during the transition of the excitation wave from viable Purkinje fibers to dead working cardiomyocytes during myocardial infarction).
3. Violation of intercellular electrotonic interactions.
4. An increase in the resistance to axial current from gap junctions as a result of an increase in the intracellular content of Ca 2+ ions (with myocardial ischemia or an overdose of cardiac glycosides).
5. Increased severity of myocardial anisotropy. Anisotropy is a property of the heart tissue to conduct an impulse differently depending on the direction of its movement. An increase in the severity of myocardial anisotropy is observed with the growth of connective tissue in the heart, as well as violations of the electrophysiological properties of the cells of the conduction system of the heart and working cardiomyocytes.
The manifestations of conduction disturbances are bradyarrhythmias or tachyarrhythmias. Bradyarrhythmias are more often observed with various heart blocks. Tachyarrhythmias are the result of (1) the appearance of accelerated escape rhythms against the background of a slowdown in the sinus node, (2) re-entry of the excitation wave - re-entry.
Pathogenesis of arrhythmias due to re-entry
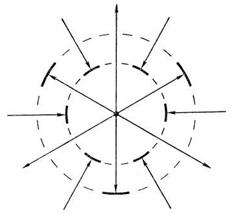
Under physiological conditions, after the generation of an impulse by the cells of the sinus node, the excitation wave propagates along the conduction system of the heart with a damped decrement. However, there are situations when the excitation wave does not die out, but recirculates, causing excitation of the myocardium. Arrhythmias, which are based on the recirculation of excitation, are caused by the re-entry mechanism - "re-entry" (English, Fig. 5). For re-entry to occur, the following conditions must be met:
Rice. 5 Schematic representation of the conditions necessary for the occurrencere- entry.
The substrate for re-entry can be almost any part of the heart. There are two types of re-entry - anatomical and functional. Anatomical re-entry is formed by morphological structures - for example, a loop of Purkinje fibers, accessory pathways, etc. Functional re-entry is much more common than anatomical and is formed by heart tissues with different electrophysiological properties. Alternative paths should have slower impulse conduction. A unidirectional impulse conduction block is observed if the impulse cannot propagate in one direction - for example, antegrade, but is able to propagate in the other direction - retrograde. This is explained by the fact that the cardiomyocytes that make up the circulation trajectory of the repeated excitation wave have different effective refractory periods. An impulse, which for some reason cannot propagate antegrade, goes by a roundabout, retrograde path. During this time, the effective refractory period of the area with a unidirectional block ends, and the excitation wave again reaches the area of the myocardium with increased automatism or trigger activity. The central zone of the impulse conduction block, around which the excitation wave circulates, is created by the anatomical features of the tissue, its functional properties, or combines these features.
It has been established that the mechanisms of re-entry of excitation underlie many rhythm disorders: paroxysmal supraventricular tachycardia with re-entry of excitation in the AV node, paroxysmal tachycardia from the AV node, with tachyarrhythmias associated with activation of congenital additional impulse conduction pathways (for example, Wolff-syndrome). Parkinson-White), atrial flutter and fibrillation, nodal rhythms from the AV junction, accelerated idioventricular rhythm, etc.
At the heart of all arrhythmias is a violation of the formation or conduction of an impulse, or a simultaneous disorder of both functions of the conduction system. Arrhythmias such as sinus tachycardia and bradycardia are associated with an increase or decrease in the automatism of the cells of the sinus node, respectively. In the origin of extrasystole and paroxysmal rhythm disturbances, 2 main mechanisms are distinguished: increased automatism of ectopic foci, re-entry of excitation (re-entry) and circular motion of the impulse.
Increased automatism of ectopic foci may be associated with acceleration or deceleration of spontaneous diastolic depolarization, fluctuations in the excitation threshold and resting potential, as well as with trace subthreshold and suprathreshold oscillations.
The mechanism of excitation re-entry (re-entry) consists in repeated or multiple excitation of a myocardial region with the same pulse, making a circular motion. To implement this mechanism, two conduction pathways are required, and one of them impairs the passage of the impulse due to local unidirectional blockade.
 The area of the myocardium, to which the next impulse did not reach in a timely manner, is excited in a roundabout way with some delay and becomes a source of extraordinary excitation. It spreads to neighboring areas of the myocardium, if these areas have managed to get out of the state of refractoriness.
The area of the myocardium, to which the next impulse did not reach in a timely manner, is excited in a roundabout way with some delay and becomes a source of extraordinary excitation. It spreads to neighboring areas of the myocardium, if these areas have managed to get out of the state of refractoriness.
The macro re-entry mechanism is possible due to the functional division of the atrioventricular node into two parts, conducting impulses at different speeds due to functioning additional pathways (in WPW syndrome), and the micro re-entry mechanism is realized mainly by anastomoses in the branches of the conducting system.
Violation of impulse conduction is primarily due to a decrease in the action potential, which may be associated with a decrease in the resting potential. Conduction disturbances can develop due to a prolongation of the refractoriness period (slow repolarization) in the areas of the conduction system.
One of the mechanisms of conduction disturbance is the so-called decremental conduction, which consists in a progressive decrease in the rate of depolarization and action potential during the propagation of an impulse from one fiber to another. An important role in the mechanism of parasystolic arrhythmias is played by the so-called blockade of entry and exit in the region of the ectopic focus.
Under the blockade of the entrance is understood the impossibility of penetration into the ectopic focus of impulses of the main rhythm, and under the blockade of the exit- the impossibility of leaving this focus of part of the ectopic impulses.
The development of combined arrhythmias may be based on a combination of the above and some other mechanisms.
"Practical electrocardiography", V.L. Doshchitsin
Cardiac arrhythmias are one of the most common manifestations of cardiovascular diseases. In recent years, significant progress has been made in the diagnosis of rhythm and conduction disorders due to the use of new methods of long-term ECG recording, electrohysography, and programmed cardiac stimulation. These methods obtained new data on the anatomy and electrophysiology of the conduction system of the heart, on the pathogenetic mechanisms of rhythm and conduction disturbances. As a result…
I. Impulse formation disorders: sinus tachycardia. sinus bradycardia. sinus arrhythmia. migration of the rhythm source. extrasystoles: supraventricular and ventricular; single, group, allorhythmic; early, middle and late; paroxysmal tachycardia: supraventricular and ventricular; according to the re-entry mechanism and ectopic; non-paroxysmal tachycardia and accelerated ectopic rhythms: supraventricular and ventricular; according to the re-entry mechanism, parasystolic and elusive; atrial flutter: paroxysmal and persistent; right...
If in the process of deciphering the ECG, signs of any rhythm or conduction disturbance are detected, then a special technique should be used. The analysis of arrhythmia should begin with the identification of P waves, their regularity and the atrial rate, which is determined in the same way as the ventricular rate. At the same time, changes in the atrial rate can be detected: its slowdown (sinus bradycardia, sinoauricular ...
You should proceed to the analysis of the ventricular rhythm: its frequency (if it was not determined earlier) and the regularity of the R-R intervals. There may be individual premature QRS complexes against the background of the correct rhythm (extrasystoles), individual prolapse of ventricular complexes due to sinoauricular or atrioventricular blockade, or completely irregular, erratic rhythm characteristic of atrial fibrillation. It is also necessary to determine the width of the QRS complexes, the position of the electrical ...